Covid-19
It is now clear that many of the deleterious effects of SARS-CoV-2 infection are caused by the presence of the viral spike protein. Alarmingly, COVID “vaccines” work by forcing the cells of the body to make the full-length, viral spike protein. Because the negative outcomes seen with COVID, Post-COVID Syndrome, and COVID vaccine injury are a result of the toxicity of the spike protein and the body’s response to it, healing modalities that address spike protein toxicity have the power to benefit all of these conditions.
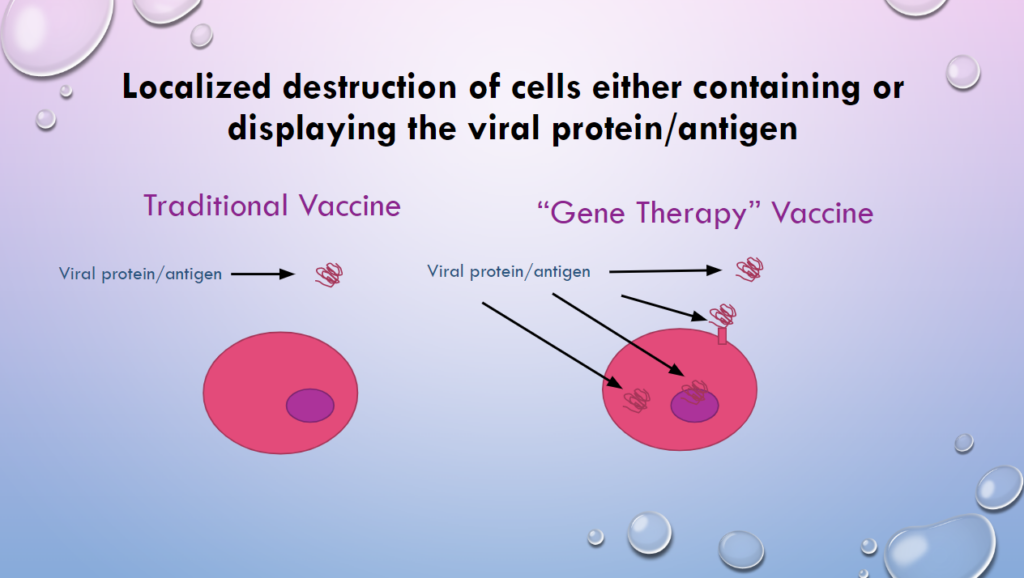
How does “gene-therapy” vaccines differ from traditional vaccines?
Traditional Vaccines
With a traditional vaccine, only a very tiny amount of protein from the bacteria or virus is injected into the muscle. This protein is recognized and “remembered” by immune cells. However, the protein remains OUTSIDE of the cells of the body until it is eaten and destroyed by immune cells. Once this happens, the protein is no longer in the body.
Gene-Therapy Vaccines
With a gene-therapy vaccine, a viral vector or a fat-like vesicle delivers genetic material into cells all over your body. Once this genetic material gets inside of your cells, it directs the cells to continuously make the foreign, pathogenic protein. So, the foreign protein is inside the cell, on the cell membrane and secreted from the cell into the lymph and blood stream. As a result, immune cells will be constantly be seeking to recognize and destroy the protein and the cells it is in. Moreover, cells in the lymph nodes will be constantly making the protein and “presenting” it to the immune system, which will result in chronic immune activation.
Concerns with gene transfer technology being used for vaccines
Most of the available vaccines for COVID utilize gene-therapy technology. Additional vaccines using the same technology are being developed, so it is critically important that we understand why this technology is NOT safe for use as a vaccine.
- Get the target genetic material into as many of the cells of interest as possible
- Have the mRNA for the gene expressed for as long as possible
- Have a much of the target protein expressed for as long as possible
Conversely, the goal of immunization is to get just enough pathogenic material into the body as necessary to provoke the immune system to develop antibodies to the foreign material. There is no need for the body to be exposed to, let alone produce large amounts of pathogenic material (antigens).
The most important thing to consider when using gene-therapy as a vaccine, is that cells are being instructed to produce a foreign, viral protein rather than a human protein. Thus, it should be expected that the immune system will target this foreign protein and the cells that produce it for destruction.
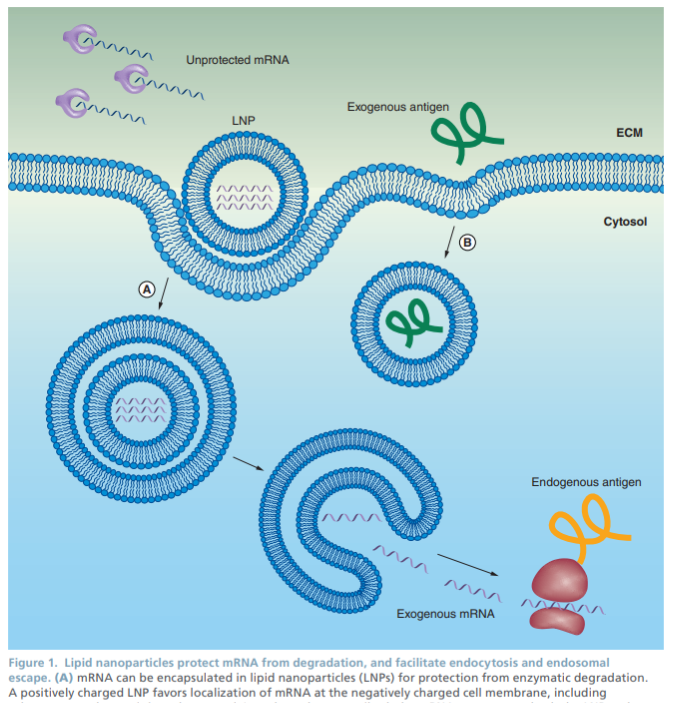
Reichmuth, andreas M et al. “mRNA Vaccine Delivery Using Lipid Nanoparticles.” Therapeutic delivery vol. 7,5 (2016): 319-34. Doi:10.4155/tde-2016-0006 https://pubmed.ncbi.nlm.nih.gov/27075952/
Christina Parks, Ph.D. Briefs the Southwest Idaho Health District Board on
Why Genetic Vaccines are NOT Safe.
Sfera A, et al. (2022) Do messenger RNA Vaccines Induce Pathological Syncytia?. Int J Pathol Clin Res 8:137. doi.org/10.23937/2469-5807/1510137 https://www.clinmedjournals.org/articles/ijpcr/international-journal-of-pathology-and-clinical-research-ijpcr-8-137.php
Pfizer / Moderna Vaccines
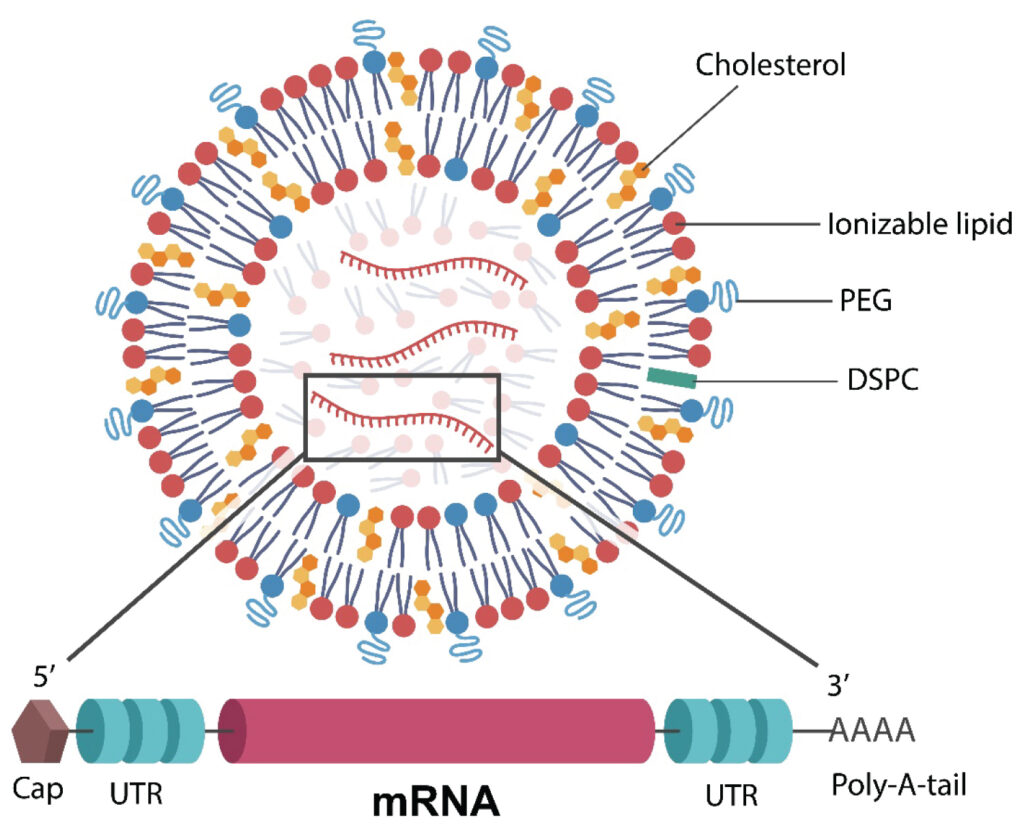
Understanding Pfizer / Moderna Vaccines
- Fat-like vesicles delivers synthetic mRNA encoding the viral Spike protein into cells, where they make, display and secrete the viral protein.
- This product is produced using a cell-free system.
- This is essentially a pseudo-virus that does not have replication capability.
Concerns with the Lipid Nanoparticles (vesicles)
- The synthetic nano-lipid vesicles are extremely inflammatory. [1-4]
- The nano-lipid vesicles are oily and accumulates in fatty areas such as the ovaries, adrenals and bone marrow.
- The lipid nano-lipid vesicles disrupt blood-brain barrier integrity. [7]
- The nano-lipid vesicles may mimic phosphatidylserine action and stimulate aberrant cell fusion. [9]
- The nano-lipid vesicles cause the unintentional activation of signaling pathways involved in inflammation and other functions. [3]
Concerns with the Synthetic mRNA
- The synthetically stabilized mRNA is more efficient than normal mRNA at producing protein. [13]
- The synthetically stabilized mRNA continues to produce a foreign, viral protein (spike) indefinitely.
- The synthetically stabilized mRNA changes the ability of the immune system to react to pathogens by downregulating the function of Toll-like receptors. [14]
References
- Reichmuth, andreas M et al. “mRNA Vaccine Delivery Using Lipid Nanoparticles.” Therapeutic delivery 7,5 (2016): 319-34. Doi:10.4155/tde-2016-0006 https://pubmed.ncbi.nlm.nih.gov/27075952/
- Ndeupen, Sonia et al. “The mRNA-LPN Platform’s Lipid Nanoparticle Component Used in Preclinical Vaccine Studies is Highly Inflammatory.” IScience 24,12 (2021): 103479. Doi:10.1016/j.Isci.2021.103479 https://pubmed.ncbi.nlm.nih.gov/34841223/
- Lonez, Caroline et al. “Cationic Lipids Activate Intracellular Signaling Pathways.” Advanced Drug Delivery Reviews 64,15 (2012): 1749-58. Doi:10.1016/j.Addr.2012.05.009 https://pubmed.ncbi.nlm.nih.gov/22634161/
- Lonez, Caroline et al. “Cationic Lipid Nanocarriers Activate Toll-Like Receptor 2 and NLRP3 Inflammasome Pathways.” Nanomedicine : Nanotechnology, Biology, and Medicine 10,4 (2014): 775-82. Doi:10.1016/j.Nano.2013.12.003 https://pubmed.ncbi.nlm.nih.gov/24361386/
- Christensen, Dennis et al. “Cationic Liposomes as Vaccine Adjuvants.” Expert Review of Vaccines 10,4 (2011): 513-21. Doi:10.1586/erv.11.17 https://pubmed.ncbi.nlm.nih.gov/21506648/
- Mohamed, Marwa et al. “Pegylated liposomes: immunological responses.” Science and technology of advanced materials 20,1 710-724. 26 jun. 2019, doi:10.1080/14686996.2019.1627174 https://pubmed.ncbi.nlm.nih.gov/31275462/
- Lockman, Paul R et al. “Nanoparticle Surface Charges Alter Blood-Brain Barrier Integrity and Permeability.” Journal of Drug Targeting 12,9-10 (2004): 635-41. Doi:10.1080/10611860400015936 https://pubmed.ncbi.nlm.nih.gov/15621689/
- Lv, Hongtao et al. “Toxicity of Cationic Lipids and Cationic Polymers in Gene Delivery.” Journal of Controlled Release : Official Journal of the Controlled Release Society 114,1 (2006): 100-9. Doi:10.1016/j.Jconrel.2006.04.014 https://pubmed.ncbi.nlm.nih.gov/16831482/
- Zhang, Zhengrong et al. “Sars-CoV-2 Spike Protein Dictates Syncytium-Mediated Lymphocyte Elimination.” Cell Death and Differentiation 28,9 (2021): 2765-2777. Doi:10.1038/s41418-021-00782-3 https://pubmed.ncbi.nlm.nih.gov/33879858/
- Sfera A, et al. (2022) Do messenger RNA Vaccines Induce Pathological Syncytia?. Int J Pathol Clin Res 8:137. doi.org/10.23937/2469-5807/1510137 https://www.clinmedjournals.org/articles/ijpcr/international-journal-of-pathology-and-clinical-research-ijpcr-8-137.php
- Alameh, Mohamad-Gabriel et al. “Messenger RNA-based Vaccines Against Infectious Diseases.” Current Topics in Microbiology and Immunology, 10.1007/82_2020_202. 17 Apr. 2020, doi:10.1007/82_2020_202 https://pubmed.ncbi.nlm.nih.gov/32300916/
- Karikó, Katalin et al. “Suppression of RNA Recognition by Toll-Like Receptors: The Impact of Nucleoside Modification and the Evolutionary Origin of RNA.” Immunity 23,2 (2005): 165-75. Doi:10.1016/j.Immuni.2005.06.008 https://pubmed.ncbi.nlm.nih.gov/16111635/
- Karikó, Katalin et al. “Incorporation of Pseudouridine into mRNA Yields Superior Nonimmunogenic Vector with Increased Translational Capacity and Biological Stability.” Molecular Therapy : The Journal of the American Society of Gene Therapy 16,11 (2008): 1833-40. Doi:10.1038/mt.2008.200 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2775451/
J & J and Astrazeneca vaccines
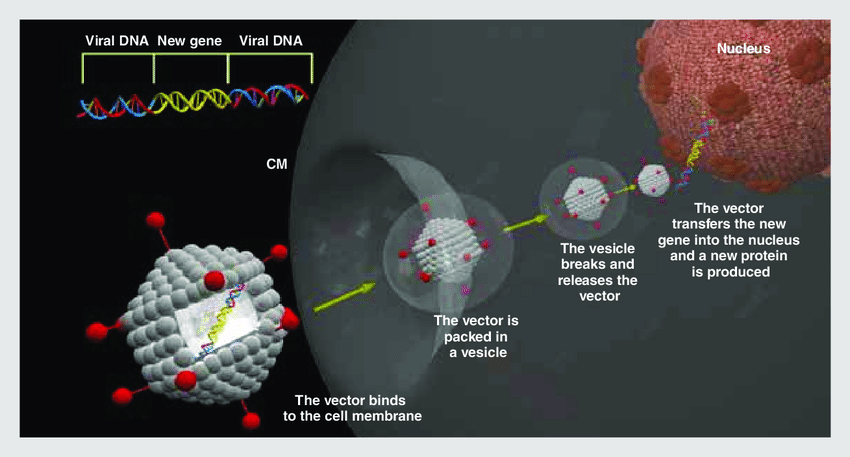
- A “disabled” human (J & J) or chimpanzee (AZ) cold virus is used to deliver DNA encoding the viral spike protein into cells. Once in cells, the DNA is copied to mRNA and then used make, display and secrete the viral spike protein.
- The “cold-virus” vectors for these vaccines are grown in cell lines derived from aborted fetuses using a “helper virus” that codes for the “cold-virus” vector.
- This gene-delivery “platform” is a pseudo-virus that contains room for several genes and has upstream regulatory elements that can control expression of those genes. It is not replication competent.
Gene therapy using an adenovirus as vector. The “new” gene (that which has to replace the mutated gene) is inserted into a viral DNA (adenovirus, lentivirus). This way, the vector will be ready to be injected into a target cell with the purpose to produce a new, functional protein. CM: cell membrane.
References
- Zhu, Feng-Cai et al. “Safety, Tolerability, and Immunogenicity of a Recombinant Adenovirus Type-5 Vectored COVID-19 Vaccine: a Dose-Escalation, Open-label, Non-Randomised, First-In-Human Trial.” Lancet (London, England) vol. 395,10240 (2020): 1845-1854. Doi:10.1016/s0140-6736(20)31208-3 https://pubmed.ncbi.nlm.nih.gov/32450106/
- Dicks, Matthew D J et al. “A Novel Chimpanzee Adenovirus Vector with Low Human Seroprevalence: Improved Systems for Vector Derivation and Comparative Immunogenicity.” Plos one vol. 7,7 (2012): e40385. Doi:10.1371/journal.Pone.0040385 https://pubmed.ncbi.nlm.nih.gov/22808149/
- Buchbinder, Susan P et al. “Use of Adenovirus Type-5 vectored Vaccines: A Cautionary Tale.” Lancet (London, England) vol. 396,10260 (2020): e68-e69. Doi:10.1016/s0140-6736(20)32156-5 https://pubmed.ncbi.nlm.nih.gov/33091364/
- Sorelle, R. “Human Gene Therapy: Science Under Fire.” Circulation vol. 101,12 (2000): e9023-4. Doi:10.1161/01.Cir.101.12.E9023 https://pubmed.ncbi.nlm.nih.gov/10736304/
- Marshall, E. “Gene Therapy Death Prompts Review of Adenovirus Vector.” Science (New York, N.Y.) Vol. 286,5448 (1999): 2244-5. Doi:10.1126/Science.286.5448.2244 https://pubmed.ncbi.nlm.nih.gov/10636774/
- Ogawara, Ken-Ichi et al. “A Novel Strategy to Modify Adenovirus Tropism and Enhance Transgene Delivery to Activated Vascular Endothelial Cells in Vitro and in Vivo.” Human Gene Therapy vol. 15,5 (2004): 433-43. Doi:10.1089/10430340460745766 https://pubmed.ncbi.nlm.nih.gov/15144574/
- Othman, Maha et al. “Adenovirus-Induced Thrombocytopenia: The Role of Von Willebrand Factor and P-Selectin in Mediating Accelerated Platelet Clearance.” Blood vol. 109,7 (2007): 2832-9. Doi:10.1182/blood-2006-06-032524 https://pubmed.ncbi.nlm.nih.gov/17148587/
- Hofherr, Sean E et al. “Polyethylene Glycol Modification of Adenovirus Reduces Platelet Activation, Endothelial Cell Activation, and Thrombocytopenia.” Human Gene Therapy vol. 18,9 (2007): 837-48. Doi:10.1089/hum.2007.0051 https://pubmed.ncbi.nlm.nih.gov/17767399/
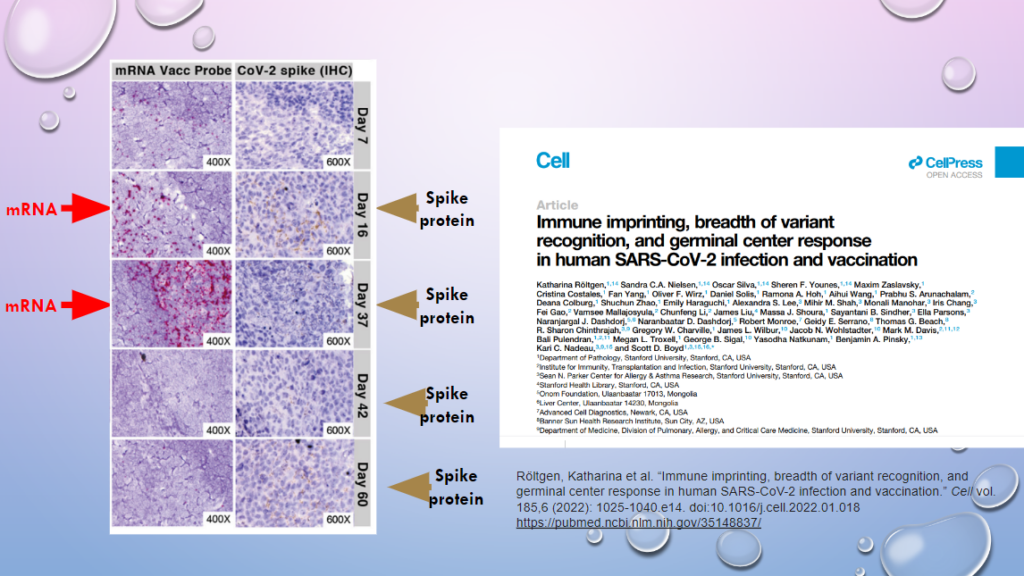
Röltgen, Katharina et al. “Immune imprinting, breadth of variant recognition, and germinal center response in human SARS-CoV-2 infection and vaccination.” Cell vol. 185,6 (2022): 1025-1040.e14. doi:10.1016/j.cell.2022.01.018 https://pubmed.ncbi.nlm.nih.gov/35148837/
Gene-therapy technology induces chronic expression of viral mRNA and spike protein
One of the key concerns of using gene-therapy technology as a vaccine is that cells in the body may continue to express foreign proteins from the pathogen, causing the body to mount a chronic immune response to destroy what it perceives as a “pathogen.”
This study from Stanford shows that vaccine-derived mRNA is abundantly present in cells from the lymph nodes of patients 37 days following vaccination and minimally present 60 days post vaccination (as evidenced by the pinkish/purple dye).
The spike protein is also being produced at both 37 and 60 days postvaccination as well, as seen by brown staining areas.
These data show the chronic production of a viral protein that induces a strong immune response from the body. This highly concerning because it will likely result in chronic inflammation as well as potential damage to tissues which are producing the spike protein.
The spike protein is present in many tissues
- Dr. Ryan Cole has found that the spike protein continues to be present in tissues many months following vaccination. Brown staining indicates the presence of the spike protein in the coronary artery, brain tissue, heart muscle and the splenic artery.
- When heart muscle is stained for both the spike protein and the nucleocapsid protein, only the spike protein is present (bottom left). The absence of the nucleocapsid protein in tissues indicates that the spike protein deposition is from vaccination and not from viral infection. This is because the vaccine does not contain genetic material to direct the production of the nucleocapsid protein, whereas the actual SARS CoV-2 virus would direct the production of both proteins as new viruses are made.

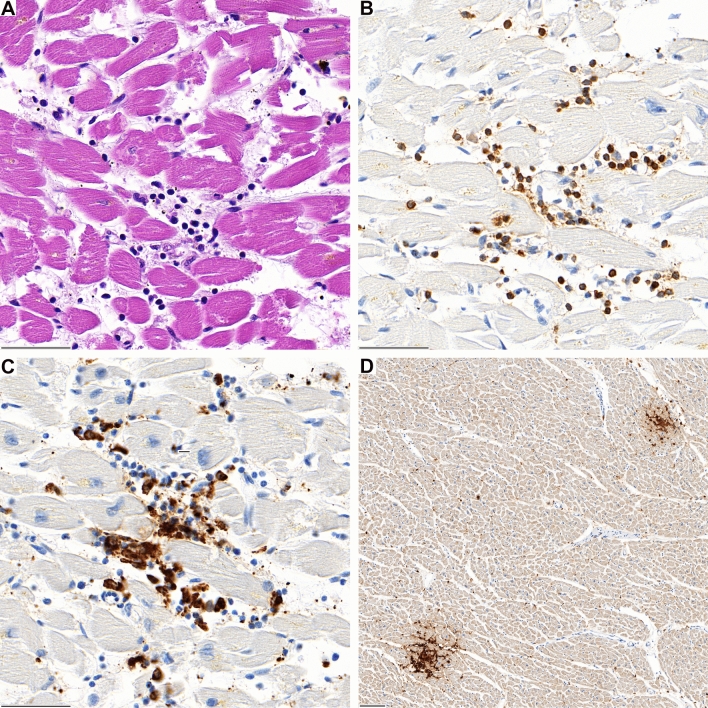
Schwab, Constantin et al. “Autopsy-based histopathological characterization of myocarditis after anti-SARS-CoV-2-vaccination.” Clinical research in cardiology : official journal of the German Cardiac Society, 1–10. 27 Nov. 2022, doi:10.1007/s00392-022-02129-5 https://pubmed.ncbi.nlm.nih.gov/36436002/
Heart tissues of some who died postvaccination are infiltrated with immune cells
- Heart tissues of several people who died within 20 days of the vaccine were infiltrated with immune cells that caused inflammation (myocarditis) and heart cell damage. The immune cells were clustered in discreet areas, consistent with the idea that they are targeting deposits of spike protein that have been produced by the cells.
- Immune cell infiltration of tissues is also associated with the expression of inflammatory cytokines, which can also contribute to inflammation/myocarditis.
Mechanisms of Injury
Medical Disclaimer: The information at vi-ta.org is presented for informational purposes only. Nothing in this website constitutes medical advice and is not intended to diagnose or prescribe for any medical or psychological condition, nor to prevent, treat, mitigate or cure such conditions. Parents, caregivers, consumers, patients, individuals and health practitioners must use their own judgment concerning specific treatment options.
vi-ta.org authors, editors, principals, partners and affiliates disclaim any liability or responsibility to any person or organization for any loss, damage, expense, fine, injury, or penalty that may arise or result from the use of any information, recommendations, opinions and/or errors on this website or in our articles, emails or links. Any use of, or reliance on, information reflected on this website, emails, articles or references is solely the responsibility of the viewer.
vi-ta.org encourages you to make your own health care decisions based on your judgment and research in partnership with a qualified healthcare professional. These statements have not been evaluated by the Food and Drug Administration. The information on this website is not intended to diagnose, treat, cure or prevent any disease.
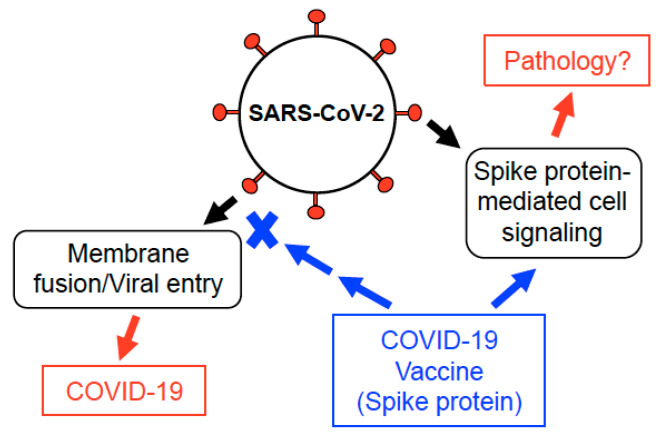
Suzuki YJ, Gychka SG. SARS-CoV-2 Spike Protein Elicits Cell Signaling in Human Host Cells: Implications for Possible Consequences of COVID-19 Vaccines. Vaccines (Basel). 2021 Jan 11;9(1):36. doi: 10.3390/vaccines9010036. PMID: 33440640; PMCID: PMC7827936.
Inflammation
One of the most serious and chronic ways that COVID and COVID vaccines injure the body is by increasing inflammation. Inflammation is very damaging to the tissues of the body and quickly depletes it of the resources necessary to maintain normal functions. Healing modalities that reduce inflammation generally or that halt one of the mechanisms of inflammation listed below will necessarily contribute to recovery. The inflammation comes from several sources:
Spike protein- the spike protein itself (whether from the vaccines or the illness) is extremely inflammatory. It binds to ACE2 receptors on cells, which begins an aberrant, inflammatory signaling cascade.[1]
Microbiome Destruction-the work of Sabin Hazan and others has documented that both COVID and the COVID vaccines have a detrimental effect on the microbiome, which results in increased inflammation. Researchers are seeing a lessening of microbiome diversity, especially with regards to Bifidobacterium and Lactobacillus species. “Good” bacteria in the gut produce anti-inflammatory molecules such as butyrate, propionate and acetate that are reduced or almost lacking in many people following vaccination or suffering from Post COVID Syndrome.[2-5]
Immune Cell Dysfunction- Certain immune cells (called non-classical monocytes) try to “clean-up” extra spike protein that is present due to illness, or resulting from vaccination, by “eating” it. However, the presence of spike protein inside these cells causes extreme dysregulation. As a result, they release large amounts of inflammatory cytokines, which draw more immune cells to the area and increase inflammation.[6]
Immune cells which become stressed, dysregulated and depleted of key anti-inflammatory molecules (such as glutathione, zinc, and Vitamin D) end up “falling apart” in a mechanism known as de-granulation. During this process, they release inflammatory signaling molecules, which draw more immune cells to the area, driving a spiral of inflammation.
In many people who have suffered from acute or chronic immune activation caused by an infection, allergen or vaccine, mast cells become chronically activated and easily triggered to release their cargo of histamine and inflammatory cytokines. This condition in which mast cells are easily activated is known as Mast Cell Activation Syndrome (MCAS). People with this syndrome begin to have easily triggered allergic-type (and even anaphylactic) responses to many foods and other elements of their environment. This process is extremely inflammatory.[7]
The nano-lipid particles in the Pfizer and Moderna vaccines, and the pseudoviral particles of the J&J and AstraZenca vaccines are all extremely inflammatory. Overcoming their inherent inflammatory nature has been one of the central challenges of gene-transfer technology.[8,9]
the goal of genetic vaccines is to get cells in the body to produce the spike protein, which the immune system then responds to. The cells that line the blood vessels are going to be among the first to take up vaccine particle and make spike protein. Once made, the spike protein will not only initiate an inflammatory response in the cells, but will also cause the immune system to target and destroy these cells, since the spike protein is foreign. This will result in massive amounts of inflammation.
References
1. Suzuki, Yuichiro J, and Sergiy G Gychka. “SARS-CoV-2 Spike Protein Elicits Cell Signaling in Human Host Cells: Implications for Possible Consequences of COVID-19 Vaccines.” Vaccines vol. 9,1 36. 11 Jan. 2021, doi:10.3390/vaccines9010036 https://pubmed.ncbi.nlm.nih.gov/33440640/
2. Papoutsis, Andreas et al. “Detection of SARS-CoV-2 from patient fecal samples by whole genome sequencing.” Gut pathogens vol. 13,1 7. 30 Jan. 2021, doi:10.1186/s13099-021-00398-5 https://pubmed.ncbi.nlm.nih.gov/33516247/
3. Giron, Leila B et al. “Plasma Markers of Disrupted Gut Permeability in Severe COVID-19 Patients.” Frontiers in immunology vol. 12 686240. 9 Jun. 2021, doi:10.3389/fimmu.2021.686240 https://pubmed.ncbi.nlm.nih.gov/34177935/
4. Hazan, Sabine et al. “Lost microbes of COVID-19: Bifidobacterium, Faecalibacterium depletion and decreased microbiome diversity associated with SARS-CoV-2 infection severity.” BMJ open gastroenterology vol. 9,1 (2022): e000871. doi:10.1136/bmjgast-2022-000871 https://pubmed.ncbi.nlm.nih.gov/35483736/
5. Wang, Huifen et al. “Potential Associations Between Microbiome and COVID-19.” Frontiers in medicine vol. 8 785496. 22 Dec. 2021, doi:10.3389/fmed.2021.785496 https://pubmed.ncbi.nlm.nih.gov/35004750/
6. Patterson, Bruce K et al. “Persistence of SARS CoV-2 S1 Protein in CD16+ Monocytes in Post-Acute Sequelae of COVID-19 (PASC) up to 15 Months Post-Infection.” Frontiers in immunology vol. 12 746021. 10 Jan. 2022, doi:10.3389/fimmu.2021.746021 https://pubmed.ncbi.nlm.nih.gov/35082777/
7. Krystel-Whittemore, Melissa et al. “Mast Cell: A Multi-Functional Master Cell.” Frontiers in immunology vol. 6 620. 6 Jan. 2016, doi:10.3389/fimmu.2015.00620 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4701915/
8. Ndeupen, Sonia et al. “The mRNA-LNP platform’s lipid nanoparticle component used in preclinical vaccine studies is highly inflammatory.” iScience vol. 24,12 (2021): 103479. doi:10.1016/j.isci.2021.103479 https://pubmed.ncbi.nlm.nih.gov/34841223
9. Mohamed, Marwa et al. “PEGylated liposomes: immunological responses.” Science and technology of advanced materials vol. 20,1 710-724. 26 Jun. 2019, doi:10.1080/14686996.2019.1627174 https://pubmed.ncbi.nlm.nih.gov/31275462/
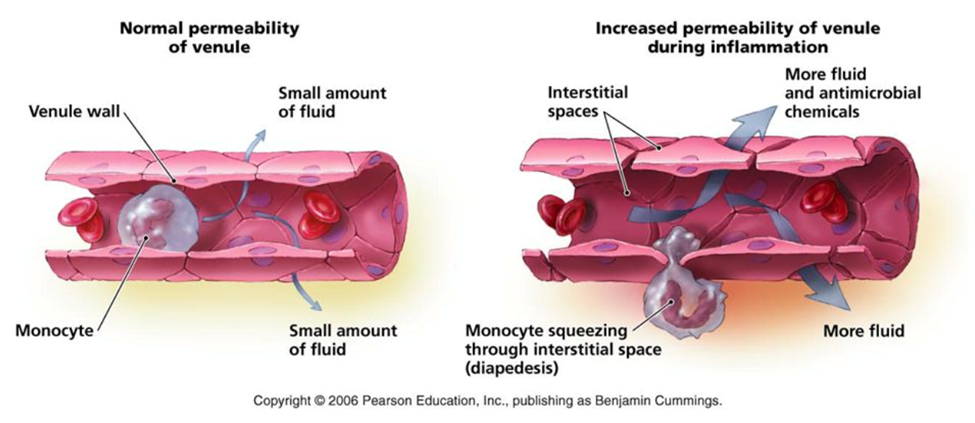
Vasculitis (Blood Vessel Inflammation)
Much of the lung damage seen in severe COVID patients is now thought to be the result of severe vasculitis in the lung tissue. Likewise, COVID vaccines are causing severe inflammation of the blood vessels through many mechanisms, many of which are listed in the “Inflammation” section. Further, the cells that line blood vessels (vascular endothelium) play a key role in immune system signaling and enact complex activities related to blood vessel dilation, permeability and blood clotting in response to immune signaling molecules. As such, they are key mediators of the inflammatory immune response and their hyperactivation and dysregulation is known to play a key role in the development of sepsis (life-threatening systemic inflammation). Here, I want to stress several important components of vasculitis that make this element of vaccine injury especially likely and pernicious.[1-4]
The goal of genetic vaccines is to get cells in the body to produce the spike protein, which the immune system then responds to. The cells that line the blood vessels are going to be among the first to take up vaccine particle and make spike protein. Once made, the spike protein will not only initiate an inflammatory response in the cells, but will also cause the immune system to target and destroy these cells, since the spike protein is foreign. Immune cells will infiltrate the areas in the blood vessel walls that are making spike protein, causing significant swelling of the blood vessels. The damage caused by cell death and immune cells targeting and “eating” cells expressing the spike protein will cause a significant weakening of the blood vessel walls, and could potentially lead to perforation or aneurysm. [5]
Mast cells activation (see Inflammation section) contributes significantly to vasculitis because histamine released by mast cells signals the blood vessels to swell (edema) and also to become permeable by weakening cell-
to-cell contacts. The function of this is to allow immune cells to move from the blood vessels into the tissue in order to deal with a perceived threat. When combined with the fact that the lining of blood vessels is already inflamed by vaccine particles, spike protein signaling and immune system targeting, mast cell activation may drive vasculitis to a critical, pathological level.[6]
References
1. Khakpour, Samira et al. “Vascular endothelial cell Toll-like receptor pathways in sepsis.” Innate immunity vol. 21,8 (2015): 827-46. doi:10.1177/1753425915606525 https://pubmed.ncbi.nlm.nih.gov/26403174/
2. Panigrahi, Soumya et al. “SARS-CoV-2 Spike Protein Destabilizes Microvascular Homeostasis.” Microbiology spectrum vol. 9,3 (2021): e0073521. doi:10.1128/Spectrum.00735-21 https://pubmed.ncbi.nlm.nih.gov/34935423/
3. Suzuki, Minami et al. “Antineutrophil Cytoplasmic Antibody-associated Vasculitis after COVID-19 Vaccination with Pfizer-BioNTech.” Internal medicine (Tokyo, Japan) vol. 61,19 (2022): 2925-2929. doi:10.2169/internalmedicine.9807-22 https://pubmed.ncbi.nlm.nih.gov/36184535/
4. Baier, Eva et al. “Dual-Positive MPO- and PR3-ANCA-Associated Vasculitis Following SARS-CoV-2 mRNA Booster Vaccination: A Case Report and Systematic Review.” Vaccines vol. 10,5 653. 21 Apr. 2022, doi:10.3390/vaccines10050653 https://pubmed.ncbi.nlm.nih.gov/35632410/
5. Röltgen, Katharina et al. “Immune imprinting, breadth of variant recognition, and germinal center response in human SARS-CoV-2 infection and vaccination.” Cell vol. 185,6 (2022): 1025-1040.e14. doi:10.1016/j.cell.2022.01.018 https://pubmed.ncbi.nlm.nih.gov/35148837/
6. Krystel-Whittemore, Melissa et al. “Mast Cell: A Multi-Functional Master Cell.” Frontiers in immunology vol. 6 620. 6 Jan. 2016, doi:10.3389/fimmu.2015.00620 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4701915/
Brian Hooker, Ph.D. Explains That the CDC knew the Vaccines Caused
Myocarditis but Withheld the Information
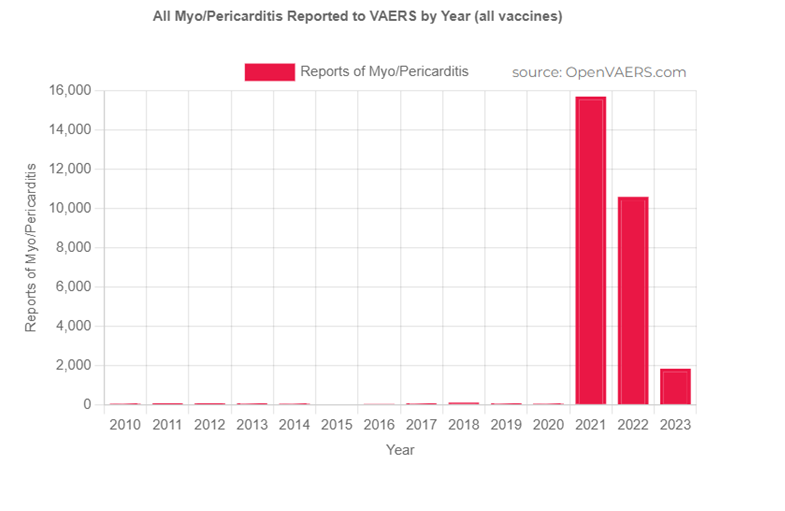
Myocarditis
The Center for Disease Control and Prevention (CDC) admits that there is a causal relationship between mRNA vaccination and the development of myocarditis (inflammation of the heart), which is highest in adolescent boys.[1] The Vaccine Adverse Event Reporting System (VAERS) currently reports over 27,000 cases of myocarditis related to the COVID 19 vaccines.[14] While epidemiological data from hospitalization data put the risk of myocarditis in teen boys at 28-150 cases per million, prospective
studies show the incidence of heart problems in teen boys to be much greater.[2-4] A prospective study is one which monitors outcomes both before and after vaccination in order to identify key changes that may be caused by vaccination. Two prospective studies showed that the incidence of myocarditis/pericarditis is closer to 1 in 50, with almost 30% of teen boys experiencing some adverse cardiac issues following vaccination. Thus, although the development of severe myocarditis requiring emergency care may be rare, mild or subclinical heart damage may be common in teen boys following mRNA vaccination. Screening for myocarditis following vaccination is important because, while mild myocarditis may resolve naturally, if the heart is stressed during this critical period, it could lead to more severe cardiac complications, including cardiac arrest. Concerningly, follow-up studies indicate that many patients with vaccine-induced myocarditis still showed myocardial deformation and late gadolinium enhancement (LGE), which is a marker or chronic inflammation and edema.[5-7] Both of these conditions are correlated with poor long-term outcomes.[8]
The nano-lipid particles in the Pfizer and Moderna vaccines are ‘fat-loving” and localize to fatty areas of the body, including adrenal glands, bone marrow, and ovaries.[13] It is likely that they also localize to the fatty tissue covering the heart. Since the nano-lipid particles are extremely inflammatory, some of the inflammation of the heart following vaccination is likely due to these particles. Further, if the fatty tissue of the heart preferentially absorbs the vaccine particles, then this tissue and the underlying heart tissue may be expressing spike protein at higher rates than other tissues.
Once made, the spike protein will not only initiate an inflammatory response in the cells, but will also cause the immune system to target and destroy these cells, since the spike protein is foreign. Myocarditis has been shown to be accompanied by immune cell infiltration which is accompanied by the release of inflammatory cytokines, causing significant swelling of the blood vessels and tissues of the heart.[10-12] The inflammation and damage to heart cells will compromise the electrical signaling that is critical to the proper contractile rhythms of the heart.[10-12] The central role of the spike protein in myocarditis is highlighted by a study showing that adolescent boys that experienced myocarditis did not make neutralizing antibodies to the spike protein following vaccination, while those who were unaffected did have circulating antibodies to the spike protein.[9]
References
1. https://www.cdc.gov/vaccines/covid-19/clinical-considerations/myocarditis.html
2. Pillay, Jennifer et al. “Incidence, risk factors, natural history, and hypothesised mechanisms of myocarditis and pericarditis following covid-19 vaccination: living
evidence syntheses and review.” BMJ (Clinical research ed.) vol. 378 e069445. 13 Jul. 2022, doi:10.1136/bmj-2021-069445 https://pubmed.ncbi.nlm.nih.gov/35830976
3. Mansanguan, Suyanee et al. “Cardiovascular Manifestation of the BNT162b2 mRNA COVID-19 Vaccine in Adolescents.” Tropical medicine and infectious disease vol. 7,8 196. 19 Aug. 2022, doi:10.3390/tropicalmed7080196 https://pubmed.ncbi.nlm.nih.gov/36006288/
4. Chiu, Shuenn-Nan et al. “Changes of ECG parameters after BNT162b2 vaccine in the senior high school students.” European journal of pediatrics vol. 182,3 (2023): 1155-1162. doi:10.1007/s00431-022-04786-0 https://pubmed.ncbi.nlm.nih.gov/36602621/
5. Yu, Clement Kwong-Man et al. “Cardiovascular Assessment up to One Year After COVID-19 Vaccine-Associated Myocarditis.” Circulation vol. 148,5 (2023): 436-439. doi:10.1161/CIRCULATIONAHA.123.064772 https://pubmed.ncbi.nlm.nih.gov/37523760/
6. Patel, Yash R et al. “Follow-Up Cardiovascular Magnetic Resonance Findings in Patients With COVID-19 Vaccination-Associated Acute Myocarditis.” JACC. Cardiovascular imaging vol. 15,11 (2022): 2007-2010. doi:10.1016/j.jcmg.2022.06.009 https://pubmed.ncbi.nlm.nih.gov/36357142/
7. Schauer, Jenna et al. “Persistent Cardiac Magnetic Resonance Imaging Findings in a Cohort of Adolescents with Post-Coronavirus Disease 2019 mRNA Vaccine Myopericarditis.” The Journal of pediatrics vol. 245 (2022): 233-237. doi:10.1016/j.jpeds.2022.03.032 https://pubmed.ncbi.nlm.nih.gov/35351530/
8. Eichhorn, Christian et al. “Multiparametric Cardiovascular Magnetic Resonance Approach in Diagnosing, Monitoring, and Prognostication of Myocarditis.” JACC. Cardiovascular imaging vol. 15,7 (2022): 1325-1338. doi:10.1016/j.jcmg.2021.11.017 https://pubmed.ncbi.nlm.nih.gov/35592889/
9. Yonker, Lael M et al. “Circulating Spike Protein Detected in Post-COVID-19 mRNA Vaccine Myocarditis.” Circulation vol. 147,11 (2023): 867-876. doi:10.1161/CIRCULATIONAHA.122.061025 https://pubmed.ncbi.nlm.nih.gov/36597886/
10. Mörz, Michael. “A Case Report: Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19.” Vaccines vol. 10,10 1651. 1 Oct. 2022, doi:10.3390/vaccines10101651 https://pubmed.ncbi.nlm.nih.gov/36298516/
11. Schwab, Constantin et al. “Autopsy-based histopathological characterization of myocarditis after anti-SARS-CoV-2-vaccination.” Clinical research in cardiology : official journal of the German Cardiac Society, 1–10. 27 Nov. 2022, doi:10.1007/s00392-022-02129-5 https://pubmed.ncbi.nlm.nih.gov/36436002/
12. Massari, Marco et al. “Postmarketing active surveillance of myocarditis and pericarditis following vaccination with COVID-19 mRNA vaccines in persons aged 12 to 39 years in Italy: A multi-database, self-controlled case series study.” PLoS medicine vol. 19,7 e1004056. 28 Jul. 2022, doi:10.1371/journal.pmed.1004056 https://pubmed.ncbi.nlm.nih.gov/35900992/
13. Pfizer Distribution Data: https://icandecide.org/wp-content/uploads/2022/03/125742_S1_M4_4223_185350.pdf
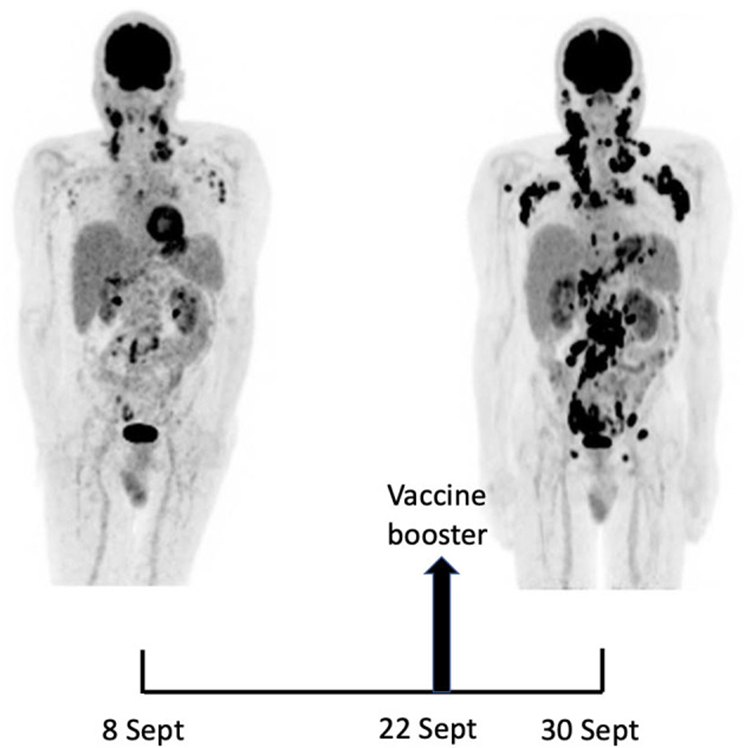
Maximum-intensity-projection images of 18F-FDG PET/CT at baseline (8 Sept) and 22 days later (30 Sept), 8 days after BNT162b2 mRNA vaccine injection in right deltoid. 8 Sept: hypermetabolic lymph nodes mainly in the supra-clavicular, cervical, and left axillary regions; restricted gastro-intestinal hypermetabolic lesions. 30 Sept: Dramatic increase in nodal and gastro-intestinal hypermetabolic lesions. Asymmetrical metabolic progression in the cervical, supra-clavicular and axillary area, more pronounced on the right side.
Goldman, Serge et al. “Rapid Progression of Angioimmunoblastic T Cell Lymphoma Following BNT162b2 mRNA Vaccine Booster Shot: A Case Report.” Frontiers in medicine vol. 8 798095. 25 Nov. 2021, doi:10.3389/fmed.2021.798095 https://pubmed.ncbi.nlm.nih.
Cancer
There are many mechanisms by which COVID vaccines may be inducing and contributing to cancer.
Recently Kevin McKernan and others verified [1] that these gene transfer vaccines were contaminated with residual DNA that is likely to be taken up by immune cells in the blood and integrated into the person’s own DNA.[2] This will cause mutations in some cells that will lead to aberrant functioning, and in some cases, cancer. Mutated blood cells which divide unchecked can result in leukemias, lymphomas and other rare blood conditions. Although more rare, insertional mutagenesis can also occur in other cell types that take up DNA from the vaccines.
The spike protein has been found to bind to the body’s major tumor suppressor gene, p53, and may inactivate it. P53 functions to make sure a cell’s DNA is intact and has no mutations prior to cell division. If the cell’s DNA is mutated beyond repair, p53 signals the cell to die (apoptosis). Inactivation of p53 leads to the proliferation of cells with increasing numbers of mutations in the DNA, which increases the likelihood that some of the cells will develop into metastatic (spreading) cancer.[3-6]
Mast cells (see Inflammation) are also involved with enhancing the formation of new blood vessels in tissues (angiogenesis). To promote new blood vessel formation, mast cells secrete signaling molecules, such as VEGF, bFGF, TGF-b, TNF-a, IL-8, and histamine. The secretion of vascular endothelial growth factor (VEGF) is known to help initiate the formation of blood vessels within tumors, a process called vascularization. Increased vascularization of tumors would be expected to fuel the growth of tumors already present in the body.[7]
COVID vaccines lead to immunosuppression by two main mechanisms. The nano-lipid particles in the mRNA vaccines were designed to downregulate the immune response of certain immune receptors, called Toll-Like Receptors (TLRs). This downregulation appears to be compromising the immune system’s ability to respond to pathogens, such as viruses and bacteria. COVID vaccines
also cause chronic immune activation which also leads to immune suppression (see Chronic Immune Activation).[7,8]
References
1. McKernan, Kevin J. et al. “Sequencing of bivalent Moderna and Pfizer mRNA vaccines reveals nanogram to microgram quantities of expression vector dsDNA per dose.” https://www.scienceopen.com/document?vid=fcbb4cb7-b0fa-46ff-9316-7cc36d51b15b
2. Ledwith, B J et al. “Plasmid DNA vaccines: investigation of integration into host cellular DNA following intramuscular injection in mice.” Intervirology vol. 43,4-6 (2000): 258-72. doi:10.1159/000053993 https://pubmed.ncbi.nlm.nih.gov/11251381/
3. Singh, Nishant, and Anuradha Bharara Singh. “S2 subunit of SARS-nCoV-2 interacts with tumor suppressor protein p53 and BRCA: an in silico study.” Translational oncology vol. 13,10 (2020): 100814. doi:10.1016/j.tranon.2020.100814 https://pubmed.ncbi.nlm.nih.gov/32619819/
4. Jiang, Hui, and Ya-Fang Mei. “SARS-CoV-2 Spike Impairs DNA Damage Repair and Inhibits V(D)J Recombination In Vitro.” Viruses vol. 13,10 2056. 13 Oct. 2021, doi:10.3390/v13102056 RETRACTED https://pubmed.ncbi.nlm.nih.gov/34696485/
5. Mirza-Aghazadeh-Attari, Mohammad et al. “53BP1: A key player of DNA damage response with critical functions in cancer.” DNA repair vol. 73 (2019): 110-119. doi:10.1016/j.dnarep.2018.11.008 https://pubmed.ncbi.nlm.nih.gov/30497961/
6. Goldman, Serge et al. “Rapid Progression of Angioimmunoblastic T Cell Lymphoma Following BNT162b2 mRNA Vaccine Booster Shot: A Case Report.” Frontiers in medicine vol. 8 798095. 25 Nov. 2021, doi:10.3389/fmed.2021.798095 https://pubmed.ncbi.nlm.nih.gov/34901098/
7. Meng, Xiao et al. “Regulatory T cells in cardiovascular diseases.” Nature reviews. Cardiology vol. 13,3 (2016): 167-79. doi:10.1038/nrcardio.2015.169 https://pubmed.ncbi.nlm.nih.gov/26525543/
8. Karikó, Katalin et al. “Suppression of RNA Recognition by Toll-Like Receptors: The Impact of Nucleoside Modification and the Evolutionary Origin of RNA.” Immunity vol. 23,2 (2005): 165-75. Doi:10.1016/j.Immuni.2005.06.008 https://pubmed.ncbi.nlm.nih.gov/16111635/
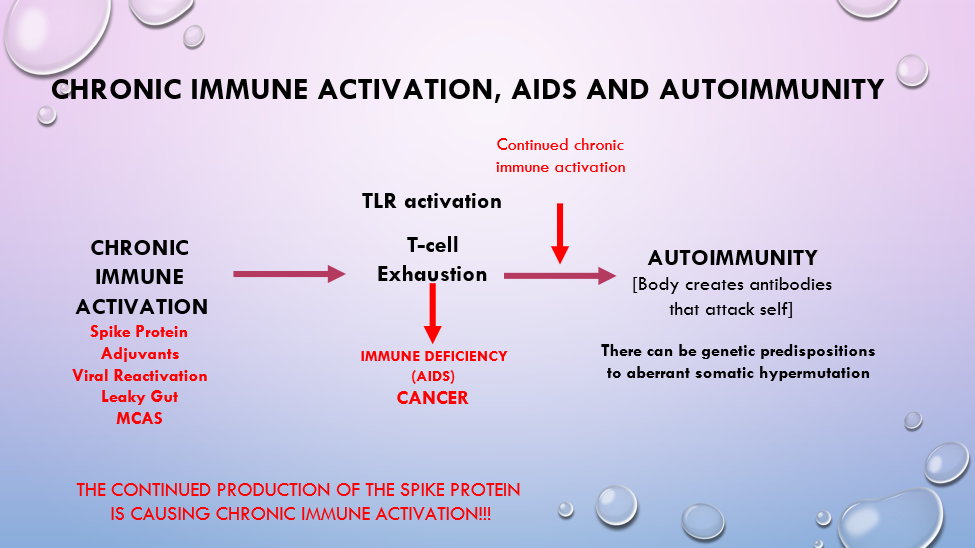
Chronic Immune Activation - Leading to Immune Suppression and Autoimmunity
COVID infection and COVID vaccination cause chronic immune activation in many individuals through a variety of mechanisms (see Inflammation). Paradoxically, when the innate immune system is chronically stimulated, it can lead to immune suppression and the development of autoimmunity. The mechanisms by which this may be occurring are now known to involve T-cells as well as certain immune receptors, known as Toll-Like Receptors (TLRs). Chronic immune activation results in T-cell dysregulation. T-cells respond to immune activation by destroying virally infected cells and cancerous cells. However, prolonged stimulation of the immune system causes T-cells to stop responding, a condition known as T-cell anergy, or T-cell exhaustion.[4] Once T-cells reach this state, they will no longer properly destroy pathogens or cancerous cells, which leaves the body in an extremely vulnerable state. Moreover, if the immune system continues to be stimulated even after T-cells are in a state of exhaustion, it causes the T-cells to become dysregulated in such a way that they induce the production of antibodies that attack the body’s own tissues.[4] The hyper-activation or hyper-expression of Toll-Like Receptors (specifically TLR7) have also been shown to play an important role in the development of autoimmunity.[11-13] Research has shown that binding of RNA, RNA/DNA hybrids, and microRNAs to TLRs (specifically TLR7) can stimulate an auto-immune response.[11-13] This is often in response to viruses and/or retroviruses in the body, but theoretically could happen in response to the RNA and/or (contaminating) DNA found in genetic vaccines.[11-13] Thus,
chronic immune activation may lead to the development of autoimmune conditions through multiple mechanisms. Further, there are many potential sources of chronic immune activation, including leaky gut, mast cell activation, chronic production of the spike protein, aluminum, and viral reactivation. Reducing chronic immune activation by addressing any of these sources may help in addressing autoimmune conditions.
References
1. Pennock, Nathan D et al. “T Cell Vaccinology: Beyond the Reflection of Infectious Responses.” Trends in immunology vol. 37,3 (2016): 170-180. doi:10.1016/j.it.2016.01.001 https://pubmed.ncbi.nlm.nih.gov/26830540/
2. Guimarães, Luísa Eça et al. “Vaccines, adjuvants and autoimmunity.” Pharmacological research vol. 100 (2015): 190-209. doi:10.1016/j.phrs.2015.08.003 https://pubmed.ncbi.nlm.nih.gov/26275795/
3. Föhse, Konstantin et al. “The impact of BNT162b2 mRNA vaccine on adaptive and innate immune responses.” Clinical immunology (Orlando, Fla.) vol. 255 (2023): 109762. doi:10.1016/j.clim.2023.109762 https://pubmed.ncbi.nlm.nih.gov/37673225/
4. Tsumiyama, Ken et al. “Self-organized criticality theory of autoimmunity.” PloS one vol. 4,12 e8382. 31 Dec. 2009, doi:10.1371/journal.pone.0008382 https://pubmed.ncbi.nlm.nih.gov/20046868/
5. Shiozawa, Shunichi et al. “DOCK8-expressing T follicular helper cells newly generated beyond self-organized criticality cause systemic lupus erythematosus.” iScience vol. 25,1 103537. 2 Dec. 2021, doi:10.1016/j.isci.2021.103537 https://pubmed.ncbi.nlm.nih.gov/34977502/
6. Holms RD. Long COVID (PASC) Is Maintained by a Self-Sustaining Pro-Inflammatory TLR4/RAGE-Loop of S100A8/A9 > TLR4/RAGE Signalling, Inducing Chronic Expression of IL-1b, IL-6 and TNFa: Anti-Inflammatory Ezrin Peptides as Potential Therapy. Immuno. 2022; 2(3):512-533. https://doi.org/10.3390/immuno2030033
7. Baeten, Dominique L P, and Vijay K Kuchroo. “How Cytokine networks fuel inflammation: Interleukin-17 and a tale of two autoimmune diseases.” Nature medicine vol. 19,7 (2013): 824-5. doi:10.1038/nm.3268 https://pubmed.ncbi.nlm.nih.gov/23836225/
8. Rose, Noel R. “Negative selection, epitope mimicry and autoimmunity.” Current opinion in immunology vol. 49 (2017): 51-55. Doi:10.1016/j.Coi.2017.08.014 https://pubmed.Ncbi.Nlm.Nih.Gov/29102863/
9. Namekata, Kazuhiko et al. “DOCK8 is expressed in microglia, and it regulates microglial activity during neurodegeneration in murine disease models.” The journal of biological chemistry vol. 294,36 (2019): 13421-13433. Doi:10.1074/jbc.Ra119.007645 https://www.Ncbi.Nlm.Nih.Gov/pmc/articles/PMC6737224/
10. Ovsyannikova, Inna G, and Gregory A Poland. “Vaccinomics: current findings, challenges and novel approaches for vaccine development.” The AA
Doi:10.1208/s12248-011-9281-x https://www.Ncbi.Nlm.Nih.Gov/pmc/articles/PMC3160164/
11. Crampton, Steve P, and Silvia Bolland. “Spontaneous activation of RNA-sensing pathways in autoimmune disease.” Current opinion in immunology vol. 25,6 (2013): 712-9. doi:10.1016/j.coi.2013.09.011 https://pubmed.ncbi.nlm.nih.gov/24455767/
12. Freund, Isabel et al. “RNA Modifications Modulate Activation of Innate Toll-Like Receptors.” Genes vol. 10,2 92. 29 Jan. 2019, doi:10.3390/genes10020092 https://pubmed.ncbi.nlm.nih.gov/30699960/
13. von Landenberg, Philipp, and Stefan Bauer. “Nucleic acid recognizing Toll-like receptors and autoimmunity.” Current opinion in immunology vol. 19,6 (2007): 606-10. doi:10.1016/j.coi.2007.10.004 https://pubmed.ncbi.nlm.nih.gov/18060756/
14. Krystel-Whittemore, Melissa et al. “Mast Cell: A Multi-Functional Master Cell.” Frontiers in immunology vol. 6 620. 6 Jan. 2016, doi:10.3389/fimmu.2015.00620 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4701915/
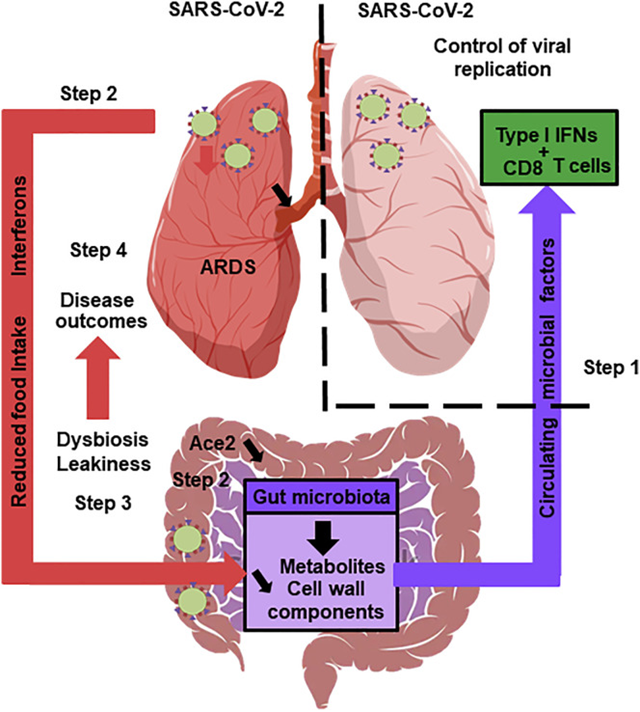
The Gut Microbiota’s Hypothetical Role in SARS-CoV-2 Infection A healthy gut microbiota boosts the lungs’ antiviral response, including interferon production and the effector function of CD8+ T cells (step 1). Soon after infection, SARS-CoV-2 replicates in the intestinal compartment and decreases the expression and activity of ACE2 (step 2). This leads to gut dysbiosis and gastrointestinal symptoms (step 3). Meanwhile, viral infection of the lungs triggers the systemic production of interferons and elicits weight loss, both of which trigger gut dysbiosis (step 3). Changes in the composition and functional activity of the gut microbiota and impairment of the gut’s barrier function contribute to disease outcomes, including ARDS, a systemic cytokine storm, and multiorgan dysfunction storm, and multiorgan dysfunction.
Trottein, François, and Harry Sokol. “Potential Causes and Consequences of Gastrointestinal Disorders during a SARS-CoV-2 Infection.” Cell reports vol. 32,3 (2020): 107915. doi:10.1016/j.celrep.2020.
Gut Dysbiosis and Leaky Gut
The gut is able to sustain an active COVID infection because intestinal cells express the ACE2 receptor that helps the virus infect cells.[1,2] In fact, researchers have shown that the rare development of Multisystem Inflammatory Syndrome (MIS-C) in children results from gut infection. In these children, infection of the gut with SARS-CoV-2 resulted in viral particles “leaking” through the gut barrier into the bloodstream, where they caused massive systemic inflammation.[4] This systemic inflammation subsided in one patient after researchers used an experimental medication to restore the integrity of the gut barrier.[4] Increased gut permeability or “leaky gut” also was associated with more severe cases of COVID in adults.[5] COVID infection and COVID vaccination are also correlated with lower levels of “good” bacteria in the gut and higher levels of opportunistic bacteria.[9,10] The resulting reductions in key species of gut bacteria, such as Bifidobacterium and Faecalibacterium are also associated with lower production of of key anti-inflammatory molecules, such as butyrate.[9,10] In addition to infecting the cells of the gut, it appears that SARS CoV-2 may be able to infect gut bacteria, thereby setting up sets up chronic infections in some people.[8] This may be a mechanism by which the virus it affects the microbiome and a potential cause of Post COVID Syndrome.[8] Sabin Hazan’s work demonstrated that therapeutics, such as vitamin C and ivermectin, aided in restoring Bifidobacterium levels.[11,12]
References
1. Lamers, Mart M et al. “SARS-CoV-2 productively infects human gut enterocytes.” Science (New York, N.Y.) vol. 369,6499 (2020): 50-54. doi:10.1126/science.abc1669 https://pubmed.ncbi.nlm.nih.gov/32358202/
2. Mönkemüller, Klaus et al. “COVID-19, coronavirus, SARS-CoV-2 and the small bowel.” Revista espanola de enfermedades digestivas vol. 112,5 (2020): 383-388. doi:10.17235/reed.2020.7137/2020 https://pubmed.ncbi.nlm.nih.gov/32343593/
3. Papoutsis, Andreas et al. “Detection of SARS-CoV-2 from patient fecal samples by whole genome sequencing.” Gut pathogens vol. 13,1 7. 30 Jan. 2021, doi:10.1186/s13099-021-00398-5 https://pubmed.ncbi.nlm.nih.gov/33516247/
4. Yonker, Lael M et al. “Multisystem inflammatory syndrome in children is driven by zonulin-dependent loss of gut mucosal barrier.” The Journal of clinical investigation vol. 131,14 (2021): e149633. doi:10.1172/JCI149633 https://pubmed.ncbi.nlm.nih.gov/34032635/
5. Giron, Leila B et al. “Plasma Markers of Disrupted Gut Permeability in Severe COVID-19 Patients.” Frontiers in immunology vol. 12 686240. 9 Jun. 2021, doi:10.3389/fimmu.2021.686240 https://pubmed.ncbi.nlm.nih.gov/34177935/
6. Trottein, François, and Harry Sokol. “Potential Causes and Consequences of Gastrointestinal Disorders during a SARS-CoV-2 Infection.” Cell reports vol. 32,3 (2020): 107915. doi:10.1016/j.celrep.2020.107915 https://pubmed.ncbi.nlm.nih.gov/32649864/
7. Petrillo, Mauro et al. “Increase of SARS-CoV-2 RNA load in faecal samples prompts for rethinking of SARS-CoV-2 biology and COVID-19 epidemiology.” F1000Research vol. 10 370. 11 May. 2021, doi:10.12688/f1000research.52540.3 https://pubmed.ncbi.nlm.nih.gov/34336189/
8. Brogna, Carlo et al. “Could SARS-CoV-2 Have Bacteriophage Behavior or Induce the Activity of Other Bacteriophages?.” Vaccines vol. 10,5 708. 29 Apr. 2022, doi:10.3390/vaccines10050708 https://pubmed.ncbi.nlm.nih.gov/35632464/
9. Hazan, Sabine et al. “Lost microbes of COVID-19: Bifidobacterium, Faecalibacterium depletion and decreased microbiome diversity associated with SARS-CoV-2 infection severity.” BMJ open gastroenterology vol. 9,1 (2022): e000871. doi:10.1136/bmjgast-2022-000871 https://pubmed.ncbi.nlm.nih.gov/35483736/
10. Wang, Huifen et al. “Potential Associations Between Microbiome and COVID-19.” Frontiers in medicine vol. 8 785496. 22 Dec. 2021, doi:10.3389/fmed.2021.785496 https://pubmed.ncbi.nlm.nih.gov/35004750/
11. Hazan, Sabine. “Microbiome-Based Hypothesis on Ivermectin’s Mechanism in COVID-19: Ivermectin Feeds Bifidobacteria to Boost Immunity.” Frontiers in microbiology vol. 13 952321. 11 Jul. 2022, doi:10.3389/fmicb.2022.952321 RETRACTED https://pubmed.ncbi.nlm.nih.gov/35898916/
12. Hazan, Sabine et al. “Vitamin C improves gut Bifidobacteria in humans.” Future microbiology, 10.2217/fmb-2022-0209. 8 Dec. 2022, doi:10.2217/fmb-2022-0209 https://pubmed.ncbi.nlm.nih.gov/36475828/

Blood Clots isolated by Dr. Ryan Cole
Blood Clots
While there may be many mechanisms by which COVID and COVID vaccines induce the formation of blood clots, it is clear that vasculitis (blood vessel inflammation) is one of the most important contributors (see Vasculitis). The cells that line blood vessels (vascular endothelium) play a key role in immune system signaling and enact complex activities related to blood vessel dilation, permeability and blood clotting in response to immune activation.[1] The dysregulated activation of immune receptors (Toll-Like Receptors-TLRs) on the surface of these endothelial cells is known to be a major contributor to pathologic blood clot formation.[1] Since SARS CoV-2 infection and COVID vaccines chronically and aberrantly activate the TLRs on cells lining the blood vessels, they cause a shift in the body toward a state of hypercoagulation, increasing the formation of blood clots.[2-4] Other factors that may increase clotting include
Mast cells release tryptase and chymase. These enzymes degrade proteins within atherosclerotic plagues, which can destabilized them and increase the incidence of blood clots (thrombotic events).[5]
The goal of genetic vaccines is to get cells in the body to produce the spike protein. Spike protein produced by immune cells and endothelial cells may contribute to clotting through several mechanisms. The spike protein has been found in blood clots, consistent with studies showing the spike protein itself can form protein aggregates.[6-8] This clotting may be stimulated in response to inflammation and the presence of bacterial cell membrane in the bloodstream.[7] Thus, clotting may be increased in persons with high levels of inflammation, leaky gut or dental infection. Other studies suggest that the spike protein is inducing the aberrant aggregation of other clotting proteins, such as fibrinogen and that the resulting clots are resistant to being broken down.[9,10]
References
1. Khakpour, Samira et al. “Vascular endothelial cell Toll-like receptor pathways in sepsis.” Innate immunity vol. 21,8 (2015): 827-46. doi:10.1177/1753425915606525 https://pubmed.ncbi.nlm.nih.gov/26403174/
2. Iba, Toshiaki, and Jerrold H Levy. “Thrombosis and thrombocytopenia in COVID-19 and after COVID-19 vaccination.” Trends in cardiovascular medicine vol. 32,5 (2022): 249-256. doi:10.1016/j.tcm.2022.02.008 https://pubmed.ncbi.nlm.nih.gov/35202800/
3. Lam, L K Metthew et al. “DNA binding to TLR9 expressed by red blood cells promotes innate immune activation and anemia.” Science translational medicine vol. 13,616
(2021): eabj1008. doi:10.1126/scitranslmed.abj1008 https://pubmed.ncbi.nlm.nih.gov/34669439/
4. Zheng, Yi et al. “SARS-CoV-2 spike protein causes blood coagulation and thrombosis by competitive binding to heparan sulfate.” International journal of biological macromolecules vol. 193,Pt B (2021): 1124-1129. doi:10.1016/j.ijbiomac.2021.10.112 https://pubmed.ncbi.nlm.nih.gov/34743814/
5. Krystel-Whittemore, Melissa et al. “Mast Cell: A Multi-Functional Master Cell.” Frontiers in immunology vol. 6 620. 6 Jan. 2016, doi:10.3389/fimmu.2015.00620 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4701915/
6. Nyström, Sofie, and Per Hammarström. “Amyloidogenesis of SARS-CoV-2 Spike Protein.” Journal of the American Chemical Society vol. 144,20 (2022): 8945-8950. doi:10.1021/jacs.2c03925 https://pubmed.ncbi.nlm.nih.gov/35579205/
7. Petrlova, Jitka et al. “SARS-CoV-2 spike protein aggregation is triggered by bacterial lipopolysaccharide.” FEBS letters vol. 596,19 (2022): 2566-2575. doi:10.1002/1873-3468.14490 https://pubmed.ncbi.nlm.nih.gov/36050806/
8. De Michele, Manuela et al. “Evidence of SARS-CoV-2 spike protein on retrieved thrombi from COVID-19 patients.” Journal of hematology & oncology vol. 15,1 108. 16 Aug. 2022, doi:10.1186/s13045-022-01329-w https://pubmed.ncbi.nlm.nih.gov/35974404/
9. Grobbelaar, Lize M et al. “SARS-CoV-2 spike protein S1 induces fibrin(ogen) resistant to fibrinolysis: implications for microclot formation in COVID-19.” Bioscience reports vol. 41,8 (2021): BSR20210611. doi:10.1042/BSR20210611 https://pubmed.ncbi.nlm.nih.gov/34328172/
10. Kell, Douglas B et al. “A central role for amyloid fibrin microclots in long COVID/PASC: origins and therapeutic implications.” The Biochemical journal vol. 479,4 (2022): 537-559. doi:10.1042/BCJ20220016 https://pubmed.ncbi.nlm.nih.gov/35195253/
The Dangers of DNA Contamination of the COVID Vaccines by Christina Parks
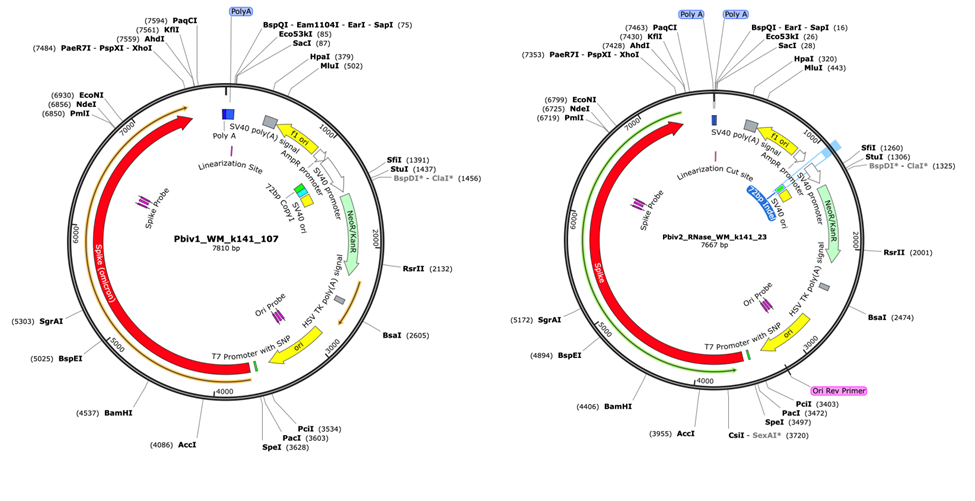
Map of the plasmid found to contaminate the Pfizer vaccine by Kevin McKernan. The plasmid contains the DNA sequence coding for the spike protein as well as a regulatory element from Simian Virus 40 (SV40) that targets DNA to the nucleus of mammalian cells, increasing risk of integration of plasmid DNA into genomic DNA.
McKernan, Kevin J. et al. “Sequencing of bivalent Moderna and Pfizer mRNA vaccines reveals nanogram to microgram quantities of expression vector dsDNA per dose.” https://www.scienceopen.com/
Kevin McKernan Briefs the Massachusetts Legislature on the Plasmid Contamination of the Pfizer Vaccine
Plasmid Contamination of Pfizer Vaccine
The work of Dr. Kevin McKernan, CSO of Medicinal Genomics, and others has demonstrated that the Pfizer vaccines are contaminated with bacterial plasmid DNA.[1] This has far-ranging implications, including that the billions of copies of fragmented DNA can be taken up by cells, where it will affect gene expression and potentially insert into the person’s DNA, causing mutations. Another important concern is that these contaminating DNA plasmids may essentially become infective agents, able to get inside both bacterial and human cells, where they direct production of the toxic foreign viral spike protein.[1] It also raises serious concerns over whether Pfizer vaccines are contaminated with bacteria endotoxins.[1]
Bacteria are used to grow up large amounts of DNA which is then used as a template to produce the mRNA for the Pfizer vaccines. This DNA is referred to as a plasmid or expression vector DNA and encodes the gene for the spike protein. It also contains several regulatory elements to “turn on” expression of the spike protein as well as genes for antibiotic resistance. The plasmid DNA is extracted from bacteria and used to make the synthetic mRNA (used for the “vaccine”) in a cell free environment. The mRNA should be extracted and purified from plasmid DNA and bacterial cell debris before being incorporated into the nano-lipid particles for the vaccine. Except, clearly, it wasn’t. Dr. McKernan’s work showed that 10-30% of the genetic material in some vials of “vaccine” was contaminating bacterial plasmid DNA.[1] If the mRNA was not properly purified and thus contains substantial amounts of bacteria DNA, the “vaccines” likely also contain residue from the bacteria themselves, in the form of bacterial endotoxins. This as well as several other serious potential health impacts are detailed below.
Contaminating bacterial endotoxins may cause anaphylaxis, severe inflammation and other vaccine injuries. One of the reasons these finding are so shocking is that contamination with bacterial toxins has plagued vaccine manufacture for decades. As it is a known problem, one would expect careful oversight of this aspect of the manufacturing process. The presence of endotoxins in a vaccine can cause anaphylaxis, severe inflammation, sepsis, endothelial fragility, bradycardia, hypotension and cardiovascular collapse, interference with energy production and such dysfunctions as Kawasaki’s Disease. All of these have been reported to VAERS following injection with the Pfizer COVID “vaccine.”[2, 3, 4, 5]
2. Plasmid DNA coding for the spike protein be incorporated into your DNA, potentially causing insertional mutagenesis. Billions of pieces of fragmented DNA were found per dose of vaccine. Alarmingly, regulatory elements within the plasmid DNA tell it to go to the nucleus of mammalian cells where it has the potential to be integrated into the person’s DNA. [6] If the plasmid inserts in a way that disrupts a key gene, it could cause insertional mutagenesis leading to dysfunction and/or cancer, especially blood cancers, such as leukemia and lymphoma.
3. Fragmented DNA and DNA/RNA hybrids may disrupt normal immune functioning and gene expression. Immune receptors respond to the presence of DNA and RNA in the body, often taking it as a sign of infection. The presence of large amounts of foreign DNA may disrupt normal immune signaling in ways that are not understood. Further, since we now know that short genetic sequences are able to affect gene expression and signal genes to be turned on or off, these sequences may be also disrupting the normal gene expression patterns in cells.
4. Spike protein may be being produced in the body in both the vaccinated and unvaccinated. Some of the contaminating bacterial DNA (plasmid) was found to be completely intact, rendering it able to enter both bacterial and human cells and potentially produce the spike protein in both cell types.[1] Thus, it is possible that people now have gut bacteria and/or human gut cells which harbor this plasmid DNA and which are making the spike protein. Once this plasmid is present in the bacteria of a person, they will then share their (potentially spike-protein producing) bacteria with
everyone they come in contact with and leave some everywhere they visit. Thus, this plasmid DNA has the potential to “infect” both the vaccinated and unvaccinated alike.
5. Development of antibiotic resistance strains of bacteria in the microbiome. The plasmids used to produce the Pfizer vaccines contain genes for antibiotic resistance (neomycin and kanamycin resistance).[1] Thus, the replication of these plasmids in our gut bacteria may contribute to the development of antibiotic resistance strains of bacteria in the microbiome.
6. Spike protein production may be amplified in people with latent SV40 viral infections. One of the regulatory elements in the plasmid is from the monkey virus, Simian Virus 40 (SV40).[1] Many people are familiar with the SV40 virus because it is a monkey virus that contaminated 10-30% of the original Polio vaccines.[7] This contamination resulted in the spread of SV40 in the population, and now it is estimated that between 1 and 15% of people may be latently infected with SV40. [8] Infected persons will produce the large T antigen protein that “turns on” the SV40 regulatory region, inducing the production of spike protein. Once made, data suggest that the spike protein may inactivate the body’s key tumor suppressor gene (p53), thereby increasing the risk of cancer.[15] Latent infection with SV40 is also known to increase cancer risk because the large T-antigen also binds and inactivates the tumor suppressor genes p53 and pRB (retinoblastoma protein). This combination may put a small, but significant portion of the population at risk for the development of “turbo cancer.”[9-13]
7. Will milk products turn on the production of spike protein in the gut? Another important regulatory region that “turns on” production of the spike protein is the T7 promoter. It is known to be “activated” in the presence of milk products. This raises the question of whether ingesting milk products will cause the gut bacteria who harbor this plasmid to start producing spike protein.[14]
While all of these are significant concerns, at this point they are largely theoretical. Studies need to be done to assess whether this plasmid is “infecting” the bacteria or cells of our gut lining. However, the important point here is that all of this should NEVER have been a concern in the first place. Pfizer should have done its due diligence in making sure that the production of the vaccine followed industry standards as well as ethical standards.
References
- McKernan, Kevin J. et al. “Sequencing of bivalent Moderna and Pfizer mRNA vaccines reveals nanogram to microgram quantities of expression vector dsDNA per dose.” https://www.scienceopen.com/document?vid=fcbb4cb7-b0fa-46ff-9316-7cc36d51b15b
- https://en.wikipedia.org/wiki/Lipopolysaccharide
- Steven M. Opal, Patrick J. Scannon, Jean-Louis Vincent, Mark White, Stephen F. Carroll, John E. Palardy, Nicolas A. Parejo, John P. Pribble, Jon H. Lemke, Relationship between Plasma Levels of Lipopolysaccharide (LPS) and LPS-Binding Protein in Patients with Severe Sepsis and Septic Shock, The Journal of Infectious Diseases, Volume 180, Issue 5, November 1999, Pages 1584–1589, https://doi.org/10.1086/315093 https://academic.oup.com/jid/article/180/5/1584/806863?login=false
- Rahmel, T., Marko, B., Nowak, H. et al.Mitochondrial dysfunction in sepsis is associated with diminished intramitochondrial TFAM despite its increased cellular expression. Sci Rep 10, 21029 (2020). https://doi.org/10.1038/s41598-020-78195-4 https://www.nature.com/articles/s41598-020-78195-4
- Takeshita, S et al. “The role of bacterial lipopolysaccharide-bound neutrophils in the pathogenesis of Kawasaki disease.” The Journal of infectious diseases 179,2 (1999): 508-12. doi:10.1086/314600 https://pubmed.ncbi.nlm.nih.gov/9878040/
- Prasad, Tekkatte Krishnamurthy, and Nalam Madhusudhana Rao. “The role of plasmid constructs containing the SV40 DNA nuclear-targeting sequence in cationic lipid-mediated DNA delivery.” Cellular & molecular biology letters 10,2 (2005): 203-15. https://pubmed.ncbi.nlm.nih.gov/16010286/
- Institute of Medicine (US) Immunization Safety Review Committee. Immunization Safety Review: SV40 Contamination of Polio Vaccine and Cancer. Edited by Kathleen Stratton et. al., National Academies Press (US), 2002. doi:10.17226/10534 https://pubmed.ncbi.nlm.nih.gov/25057632/
- Barbanti-Brodano, Giuseppe et al. “Simian virus 40 infection in humans and association with human diseases: results and hypotheses.” Virology 318,1 (2004): 1-9. doi:10.1016/j.virol.2003.09.004 https://pubmed.ncbi.nlm.nih.gov/15015494/
- Vilchez, Regis A, and Janet S Butel. “Emergent human pathogen simian virus 40 and its role in cancer.” Clinical microbiology reviews 17,3 (2004): 495-508, table of contents. doi:10.1128/CMR.17.3.495-508.2004 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC452549/
- Moreau, P et al. “The SV40 72 base repair repeat has a striking effect on gene expression both in SV40 and other chimeric recombinants.” Nucleic acids research 9,22 (1981): 6047-68. doi:10.1093/nar/9.22.6047 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC327583/
- The Simian Virus 40 Minimal Origin and the 72-Base-Pair Repeat are Required Simultaneously for Efficient Induction of Late Gene Expression with Large Tumor Antigen Stephen W. Hartzell, Barry J. Byrne and Kiranur N. Subramanian Proceedings of the National Academy of Sciences of the United States of America 81, No. 20, [Part 1: Biological Sciences] (Oct. 15, 1984), pp. 6335-6339 (5 pages) https://www.jstor.org/stable/24873
- Green, J et al. “72-bp element contains a critical control region for SV40 late expression in Xenopus laevis oocytes.” Virology 159,2 (1987): 339-49. doi:10.1016/0042-6822(87)90472-7 https://pubmed.ncbi.nlm.nih.gov/3039731/
- Martini, F et al. “SV40 early region and large T antigen in human brain tumors, peripheral blood cells, and sperm fluids from healthy individuals.” Cancer research 56,20 (1996): 4820-5. https://pubmed.ncbi.nlm.nih.gov/8841004/
- https://en.wikipedia.org/wiki/T7_expression_system
- Singh, Nishant, and Anuradha Bharara Singh. “S2 subunit of SARS-nCoV-2 interacts with tumor suppressor protein p53 and BRCA: an in silico study.” Translational oncology 13,10 (2020): 100814. doi:10.1016/j.tranon.2020.100814 https://pubmed.ncbi.nlm.nih.gov/32619819/
Dr. James Thorp Briefs the Southwest Idaho Health District Board on the
Reproductive Harms of COVID Vaccines.
Reproductive Issues
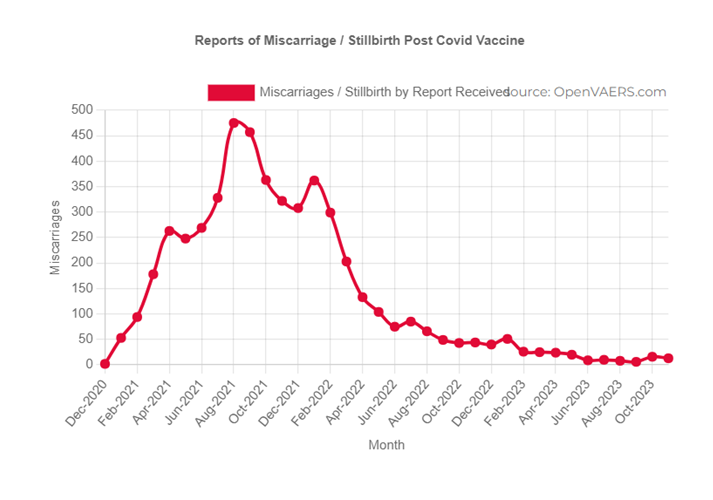
Reports of reproductive issues ranging from heavy bleeding or missed cycles to increased rates of miscarriage have followed the rollout of the COVID vaccines. The Vaccine Adverse Event Reporting System (VAERS) currently reports over 5000 miscarriages and over 37,000 reports of menstrual disorders related to the COVID 19 vaccines. Rates of stillbirth have also skyrocketed from the normal number of around 6 stillbirths per 1000 live births to 30 stillbirths/1000 live births in one area of California and an alarming 160 stillbirths/1000 live births in a hospital in Canada.[3]
COVID vaccination is extremely inflammatory and inflammation can worsen issues that affect reproduction, such as polycystic ovarian syndrome (PCOS), hypertension, stress hormone production, and general oxidative stress. Further, the fatty nano-lipid particles of the vaccine preferentially target the fatty ovaries, where they are likely to cause significant inflammation.[9] This may disrupt the production of hormones as well as eggs in the ovaries, thereby also disrupting the menstrual cycle.
It has been hypothesized that COVID vaccination may cause the production of antibodies to the viral spike protein that also cross react with the syncytin protein, since it is of viral origin. Syncytin plays a critical role in the placenta and in fertilization. However, initial studies suggest that is not playing a role in COVID vaccination-induced reproductive issues.[10,11]
One study has shown that infants born to mothers who had COVID during pregnancy had depleted numbers of blood stem cells (the cells which make all other immune and blood cells). Mothers who were vaccinated during pregnancy had infants who had almost no blood stem cells (as obtained from cord blood). Infants with severe depletions in their numbers of stem cells may suffer from severe anemia as well as have compromised immune function. It will be important to assess whether this observed depletion in stem cells is related to increases in stillbirths following vaccination.[12]
References
1. https://openvaers.com/covid-data/reproductive-health
2. Parotto, T., Thorp, J.A., Hooker, B., Mills, P.J., Newman, J., Murphy, L., Geick, W., Mcdyer, D., Stricker, R.B., Peters, S.E., McDonnell, M., Ray, H., & Northrup, C. (2022). COVID-19 and the surge in Decidual Cast Shedding. The Gazette of Medical Sciences. https://www.semanticscholar.org/paper/COVID-19-and-the-surge-in-Decidual-Cast-Shedding-Parotto-Thorp/2a6a540116aa004dfe082af4d013ba299d02e01d
3. Thorp, J.A.; Rogers, C.; Deskevich, M.P.; Tankersley, S.; Benavides, A.; Redshaw, M.D.; McCullough, P.A. COVID-19 Vaccines: The Impact on Pregnancy Outcomes and Menstrual Function.Journal of American Physicians and Surgeons. https://www.jpands.org/vol28no1/thorp.pdf
4. Lee, Katharine M N et al. “Investigating trends in those who experience menstrual bleeding changes after SARS-CoV-2 vaccination.” Science advances vol. 8,28 (2022): eabm7201. doi:10.1126/sciadv.abm7201 https://pubmed.ncbi.nlm.nih.gov/35857495/
5. Lessans, Naama et al. “The effect of BNT162b2 SARS-CoV-2 mRNA vaccine on menstrual cycle symptoms in healthy women.” International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics vol. 160,1 (2023): 313-318. doi:10.1002/ijgo.14356 https://pubmed.ncbi.nlm.nih.gov/35856178/
6. Rodríguez Quejada, Luisa et al. “Menstrual cycle disturbances after COVID-19 vaccination.” Women’s health (London, England) vol. 18 (2022): 17455057221109375. doi:10.1177/17455057221109375 https://pubmed.ncbi.nlm.nih.gov/35796571/
7. Pourmasumi, Soheila et al. “Effects of COVID-19 Infection and Vaccination on the Female Reproductive System: A Narrative Review.” Balkan medical journal vol. 40,3 (2023): 153-164. doi:10.4274/balkanmedj.galenos.2023.2023-3-4 https://pubmed.ncbi.nlm.nih.gov/37114907/
8. Saleh Alzahrani, Hayat et al. “The effect of COVID-19 vaccination on the menstrual cycle in female in Riyadh, Saudi Arabia.” Saudi pharmaceutical journal : SPJ : the official publication of the Saudi Pharmaceutical Society vol. 31,5 (2023): 746-751. doi:10.1016/j.jsps.2023.03.015 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10063452/ 9. Pfizer Distribution Data: https://icandecide.org/wp-content/uploads/2022/03/125742_S1_M4_4223_185350.pdf
10. Kloc, Malgorzata et al. “Exaptation of Retroviral Syncytin for Development of Syncytialized Placenta, Its Limited Homology to the SARS-CoV-2 Spike Protein and Arguments against Disturbing Narrative in the Context of COVID-19 Vaccination.” Biology vol. 10,3 238. 19 Mar. 2021, doi:10.3390/biology10030238 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8003504/
11. Mattar, Citra N Z et al. “BNT162B2 COVID-19 mRNA vaccination did not promote substantial anti-syncytin-1 antibody production nor mRNA transfer to breast milk in an
exploratory pilot study.” Annals of the Academy of Medicine, Singapore vol. 51,5 (2022): 309-312. doi:10.47102/annals-acadmedsg.2021447 https://pubmed.ncbi.nlm.nih.gov/35658155/
12. Estep, Benjamin K et al. “Skewed fate and hematopoiesis of CD34+ HSPCs in umbilical cord blood amid the COVID-19 pandemic.” iScience vol. 25,12 (2022): 105544. doi:10.1016/j.isci.2022.105544 https://pubmed.ncbi.nlm.nih.gov/36406860/
Become a Member of VI-TA and support us in finding answers and passing them along to those who need them most!
(for less than the price of 2 cups of coffee a month)
Why Join VI-TA?
Practitioner Presentations
Join us twice a month to hear leaders in the field share cutting edge information on what is working to help their patients.
Support on Your Healing Journey
Have information that supports your healing journey at your fingertips when you need it.
Protocols for Healing
Links to the most up-to-date protocols for helping the body recover from vaccine injury and toxic overload.
Learn About Healing Modalities
Learn the pros and cons of different healing modalities and which may be best to support your healing journey.


VACCINE INJURY TEACHING ALLIANCE
Empowering people with the information they need to maintain and restore health in this age of toxic overload, mass vaccination, and skyrocketing chronic illness.
Contact Us
VACCINE INJURY TEACHING ALLIANCE
Empowering people with the information they need to maintain and restore health in this age of toxic overload, mass vaccination, and skyrocketing chronic illness.
Contact Us
- Presentations & Events
- Our Practitioners
- FAQs
- Members Login
- Donate